
Hospitals are among the most complex and high-risk environments for fire emergencies in the entire built environment. Patients who are sedated, on life support, or otherwise unable to self-evacuate depend entirely on the reliability of the building’s fire detection and notification infrastructure. Hospital fire alarm systems must therefore meet an exceptionally rigorous set of federal, state, and accreditation standards far more demanding than those applied to standard commercial buildings. Understanding and implementing these requirements is not optional; it is a matter of life and safety for some of the most vulnerable people in any community.
In this comprehensive guide, we will walk through everything facility managers, biomedical engineers, fire safety officers, and hospital administrators need to know about fire safety requirements for healthcare environments. From the governing codes and standards to the specific devices and system architectures required, this article provides a thorough foundation for building and maintaining a compliant, reliable fire protection ecosystem in any healthcare setting.
Why Fire Safety in Healthcare Facilities Demands Special Attention
The fire risk profile of a hospital is fundamentally different from that of an office building, retail space, or even a school. Healthcare facilities contain a unique combination of hazards: medical-grade oxygen systems, flammable anesthetics, large quantities of electrical equipment, laboratory chemicals, and kitchens operating around the clock. Simultaneously, a significant portion of the occupant population is bedridden, sedated, or otherwise physically incapable of responding to an alarm and evacuating without direct staff assistance.
This combination of elevated ignition risk and diminished occupant mobility is precisely why hospital fire alarm systems are governed by layers of overlapping regulations that go well beyond the baseline requirements of the International Building Code or NFPA 72. Regulatory bodies including the Centers for Medicare and Medicaid Services (CMS), The Joint Commission, state health departments, and local authorities having jurisdiction (AHJ) all have a role in defining what is expected of a healthcare facility’s fire protection infrastructure.
Furthermore, the consequences of a fire safety failure in a healthcare environment extend beyond the immediate threat to life. A fire-related incident can trigger federal funding suspension, loss of accreditation, civil litigation, and irreparable reputational damage. Proactive, thorough compliance is therefore both a moral and a strategic imperative for every healthcare organization.
The Governing Codes and Standards for Healthcare Fire Safety
No single document defines all fire safety requirements for healthcare facilities. Instead, a layered framework of codes, standards, and accreditation requirements work in concert to establish what is required. Facility managers must be familiar with all of them.
NFPA 101 Life Safety Code
The NFPA 101 Life Safety Code is the single most important document governing fire safety in healthcare occupancies in the United States. It establishes the requirements for construction, protection, and occupancy features necessary to minimize danger from fire, smoke, fumes, or panic. For healthcare occupancies specifically, NFPA 101 Chapter 18 (new construction) and Chapter 19 (existing buildings) provide detailed requirements for compartmentalization, sprinkler systems, smoke barriers, corridor widths, and fire alarm systems.
The Centers for Medicare and Medicaid Services has formally adopted NFPA 101 as the standard against which it evaluates facilities seeking or maintaining Medicare and Medicaid certification. Non-compliance with the NFPA 101 Life Safety Code can result in a Condition of Participation deficiency, which may ultimately lead to exclusion from federal healthcare programs a financially devastating outcome for any hospital.
NFPA 72: National Fire Alarm and Signaling Code
While NFPA 101 establishes the occupancy-level requirements, NFPA 72 provides the technical specifications for how fire alarm systems must be designed, installed, tested, and maintained. All hospital fire alarm systems must comply with NFPA 72, which governs everything from wiring configurations and device placement to testing intervals and documentation requirements. NFPA 72 is updated on a triennial cycle, and jurisdictions may be enforcing different editions, so it is essential to verify which version applies in your location.
The Joint Commission Fire Safety Standards
For hospitals that seek or maintain Joint Commission accreditation, the Joint Commission fire safety standards add another layer of requirements on top of NFPA 101 and NFPA 72. The Joint Commission conducts unannounced on-site surveys and evaluates fire safety through its Environment of Care (EC) and Life Safety (LS) chapters. Key elements reviewed include the fire alarm system inspection and testing records, staff fire safety training documentation, and the results of fire drills conducted across all shifts.
The Joint Commission fire safety standards also require hospitals to maintain a written fire safety management plan and to conduct an annual review of that plan. Any deficiencies identified during a survey must be remediated on a defined timeline, and evidence of corrective action must be documented and available for review.
Core Components of Hospital Fire Alarm Systems
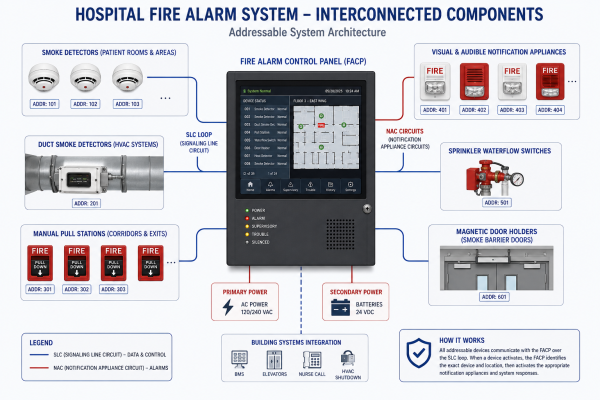
Modern hospital fire alarm systems are sophisticated, multi-component architectures designed to detect a fire in its earliest stages, notify occupants and staff, trigger protective actions such as door closure and HVAC shutdown, and communicate with the fire department all within seconds. Understanding each component and its specific role is essential to evaluating whether a system meets applicable standards.
Fire Alarm Control Panel
The fire alarm control panel hospital infrastructure centers on is the nerve center of the entire fire detection and notification system. In a healthcare setting, the FACP must support full addressability, meaning each individual device on the system can be identified by its precise location on the panel’s display. This capability is critical in a large hospital where a fire in a specific patient room, corridor, or utility space must be instantly identifiable without ambiguity. QuickShipFire offers a wide range of addressable fire alarm control panels from leading manufacturers including Notifier, Fire-Lite, and Simplex that are well-suited for healthcare applications.
The fire alarm control panel hospital administrators depend on must also provide redundant communication pathways to the monitoring station and the local fire department. Dual-path communication combining a digital dialer with a network-based communicator is increasingly required by authorities having jurisdiction to ensure that alarm signals reach emergency responders even if one communication pathway fails.
Smoke Detectors for Hospitals
Selecting the right smoke detectors for hospitals requires careful consideration of the unique environmental conditions found in healthcare settings. Patient rooms, operating theaters, and intensive care units often have elevated humidity, airborne particulates from nebulizers, or steam from sterilization equipment all of which can cause nuisance alarms with standard photoelectric or ionization detectors. Multi-criteria detectors that analyze multiple sensing parameters simultaneously are typically preferred in clinical areas to minimize false activations without compromising detection sensitivity.
Duct smoke detectors represent another critical component in hospitals with centralized HVAC systems. These devices monitor the airflow within return air ducts and trigger HVAC shutdown when smoke is detected, preventing smoke from being circulated throughout the building. QuickShipFire carries an extensive selection of duct detectors that meet NFPA 90A installation requirements and are compatible with leading addressable fire alarm panels. When choosing smoke detectors for hospitals, always verify compatibility with your control panel’s communication protocol.
Addressable Fire Alarm System Architecture
An addressable fire alarm system assigns a unique address to every detector, pull station, module, and notification appliance on the network. In a hospital with hundreds or thousands of devices spread across multiple floors and wings, this architecture is not merely preferred it is essential. When an alarm is triggered, the control panel immediately identifies the exact device and location, enabling staff to respond with pinpoint precision rather than searching an entire floor.
Beyond detection, an addressable fire alarm system also enables sophisticated control functions such as selective notification (alerting only the affected zone and adjacent staff areas), phased evacuation sequencing, elevator recall, and automatic door release. These capabilities are particularly important in healthcare settings where a full building-wide alarm could cause dangerous patient movement and panic.
Required Fire Alarm Devices and Where They Must Be Located
NFPA 72 and NFPA 101 together define where specific fire alarm devices must be installed in a healthcare occupancy. Here are the key placement requirements every facility manager must know:
- Patient sleeping rooms: Require smoke detectors within each room, positioned to detect smoke before it reaches the corridor. Visual notification devices are also required for hearing-impaired patients per ADA standards.
- Corridors: Must have smoke detectors spaced no more than 30 feet apart (measured from the end of the corridor) and audible/visual notification appliances at regular intervals to ensure coverage throughout egress paths.
- Nurses stations and staff areas: Must be equipped with notification appliances and, where applicable, annunciator panels that display alarm status for the zones they oversee.
- Mechanical and electrical rooms: All rooms containing HVAC equipment, electrical panels, or fuel-burning appliances must have heat or smoke detectors as appropriate to the environment.
- Operating rooms and procedure areas: Special attention is required due to the presence of flammable anesthetic agents. Detectors must be selected to minimize nuisance alarms while maintaining sensitivity to real combustion events.
Healthcare Facility Evacuation Planning and Fire Alarm Integration
A fire alarm system is only as effective as the evacuation and response plan that it triggers. In a healthcare setting, the healthcare facility evacuation plan must account for the complexity of moving non-ambulatory patients, patients on supplemental oxygen, patients connected to monitoring equipment, and patients in sterile procedural environments. This is why healthcare facilities do not typically execute full building evacuations instead, they use a defend-in-place strategy supported by compartmentalization.
The defend-in-place approach relies on the building’s fire and smoke compartmentalization to confine a fire to a limited area while staff move patients to adjacent safe zones within the same floor. The healthcare facility evacuation plan must be documented, regularly reviewed, and practiced through fire drills conducted on all shifts. NFPA 101 requires quarterly fire drills for healthcare occupancies, with at least one drill per shift per year. Drill records must be maintained and made available to inspectors and accreditation surveyors.
The fire alarm system must be integrated with the evacuation plan in specific ways. Alarm signals must trigger automatic actions such as releasing magnetic door holders on smoke barrier doors, recalling elevators to the ground floor, and activating stairwell pressurization systems. All of these integrations depend on the capabilities of the fire alarm control panel and the quality of the hospital fire alarm systems modules installed throughout the facility.
Fire Suppression Systems in Hospitals
While fire alarm systems detect and notify, fire suppression systems in hospitals actively work to extinguish or control a fire before it can spread. Automatic sprinkler systems are required throughout virtually all new healthcare construction under NFPA 101, and their integration with the fire alarm system is essential to a complete fire protection strategy.
In a fully sprinklered healthcare facility, the fire alarm system must be interconnected with the sprinkler system so that the activation of any sprinkler head triggers an immediate alarm. This is accomplished through waterflow switches installed on each sprinkler branch line, which send a signal to the fire alarm control panel when water begins to flow. The panel then initiates the appropriate alarm sequence based on the programmed response for that zone.
Beyond standard wet-pipe sprinkler systems, many areas of a hospital require specialized fire suppression systems in hospitals, including clean agent suppression for server rooms, data centers, and imaging equipment areas; pre-action systems in MRI suites to protect against accidental discharge; and dry chemical systems in commercial kitchen areas. Each of these specialty suppression systems must be individually monitored by the fire alarm system to provide complete protection.
Key Technical Requirements for Hospital Fire Alarm Systems
The following technical specifications represent the minimum requirements that must be met by hospital fire alarm systems under applicable federal and NFPA standards. Facility managers should treat these as a baseline, not a ceiling:
- System type: Fully addressable systems are required for all new construction and major renovations in healthcare occupancies.
- Power supply redundancy: Systems must include a primary power supply (typically 120V AC) and a secondary backup (sealed lead-acid or lithium batteries) capable of powering the system for a minimum of 24 hours in standby and 5 minutes in full alarm.
- Notification appliances: Must provide both audible and visual notification throughout all occupied areas, with device spacing and intensity meeting the requirements of NFPA 72 and ADA accessibility standards.
- Communication pathways: Dual-path communication to a UL-listed central monitoring station is required, with automatic failover between primary and secondary paths.
- Wiring class: Class A wiring (Style 6 or 7 for initiating device circuits; Style Z for signaling line circuits) is strongly recommended in healthcare settings to maintain system integrity during a fire event even if a single wiring fault occurs.
- Testing and inspection: All system components must be tested and inspected in accordance with NFPA 72 Table 14.4.5, with records maintained for a minimum of three years.
Healthcare Fire Safety Requirements: Inspection, Testing, and Maintenance
Installing a compliant hospital fire alarm systems infrastructure is only the beginning. Ongoing inspection, testing, and maintenance (ITM) are mandatory under NFPA 72 and are a primary focus of Joint Commission surveys, state health department inspections, and CMS certifications. A fire alarm system that was compliant at installation but has fallen into disrepair due to inadequate maintenance represents a serious legal and safety liability.
Annual Inspection Requirements
NFPA 72 requires that all components of a fire alarm system be visually inspected annually, with functional testing performed at the frequencies specified in NFPA 72 Table 14.4.5. For healthcare occupancies, the inspection and testing program must be documented in detail, including the identity of the technician, the devices tested, the results of each test, and any corrective actions taken. These records must be available for review by any authority having jurisdiction.
Quarterly and Monthly Checks
Beyond the annual inspection, certain components of hospital fire alarm systems require more frequent attention. Battery systems must be tested quarterly. Waterflow alarms and supervisory signals from sprinkler systems must be tested semi-annually. Manual pull stations must be tested annually, and certain types of detectors including multi-criteria and aspirating detectors may have manufacturer-recommended testing intervals that are more frequent than the NFPA 72 minimums.
Device Replacement and End-of-Life Planning
Fire alarm devices have finite service lives. Smoke detectors, in particular, have a recommended replacement interval of ten years from the date of manufacture under NFPA 72. In a large hospital where hundreds or thousands of detectors may be installed, managing device replacement on a rolling basis is a significant operational and budgetary challenge. QuickShipFire specializes in sourcing hard-to-find and obsolete fire alarm components, making it possible to maintain aging systems with exact-match replacement parts while a comprehensive system upgrade is planned and funded.
Is your hospital’s fire alarm system due for inspection, device replacement, or a full upgrade? Browse QuickShipFire’s complete inventory of fire alarm panels, detectors, and notification devices all brand new in original manufacturer packaging, with fast U.S. shipping and expert technical support to keep your facility compliant and protected.
The Role of Staff Training in Healthcare Fire Safety
Even the most technically advanced hospital fire alarm systems cannot compensate for inadequately trained staff. In a healthcare environment, every clinical and non-clinical employee plays a role in fire safety response. The acronym RACE Rescue, Alarm, Contain, Extinguish or Evacuate is the standard framework used to train hospital staff on their individual responsibilities when a fire alarm is activated.
NFPA 101 requires healthcare facilities to conduct fire drills on every shift, at least four times per year. These drills must be unannounced, realistic, and evaluated. Staff must demonstrate familiarity with the location of pull stations, fire extinguishers, and smoke barrier doors, as well as the procedures for moving patients to areas of refuge. Drill records must be maintained and are routinely reviewed during Joint Commission surveys and state health department inspections.
Staff training should also include familiarization with the fire alarm control panel annunciator and the meaning of different alarm signals. In hospitals that use a zoned alarm notification strategy where only affected areas are initially notified staff in neighboring zones must understand that a local alarm in their area means they should prepare for potential patient movement even before a general evacuation is ordered.
Common Fire Safety Compliance Gaps in Healthcare Facilities
Even well-resourced hospitals can develop compliance gaps over time due to system aging, facility renovations, or staff turnover. Here are the most frequently cited fire safety deficiencies in healthcare facility inspections:
- Propped-open smoke barrier doors: One of the most common and dangerous compliance violations, often cited in both Joint Commission surveys and CMS inspections. Automatic door-closing mechanisms integrated with the fire alarm system must be tested and maintained to function reliably.
- Missing or expired detector testing records: Failure to maintain complete, up-to-date inspection and testing documentation is a routine finding during regulatory surveys and can result in immediate citations.
- Unapproved modifications to fire alarm wiring: Any changes to the fire alarm system must be performed by a licensed fire alarm contractor and documented. Unauthorized modifications can void system listings and create serious liability.
- Inadequate coverage in renovated areas: When a hospital renovates patient rooms, corridors, or clinical spaces, the fire alarm system must be updated to reflect the new layout. Detectors and notification appliances from the prior configuration may no longer provide adequate coverage.
- Incorrect device substitutions: Replacing a failed device with a non-compatible substitute even one that appears physically similar can disrupt the addressable communication protocol and create blind spots in system coverage.
Selecting the Right Equipment for Hospital Fire Alarm Systems
Sourcing reliable, compliant equipment is one of the most important decisions a healthcare facility fire safety officer will make. The performance of hospital fire alarm systems depends entirely on the quality and compatibility of the individual components from the control panel to the last notification appliance on the circuit. Here are the most important selection criteria to apply:
Manufacturer Reputation and UL Listing
All fire alarm devices installed in a healthcare facility must be listed by a nationally recognized testing laboratory (NRTL) in most cases, Underwriters Laboratories (UL). The UL listing confirms that the device has been independently tested and found to meet applicable performance standards. Purchasing from reputable, established manufacturers and from authorized or well-vetted resellers is essential to ensuring that the devices you install carry legitimate listings.
System Compatibility and Protocol Matching
Addressable fire alarm devices communicate with the control panel using proprietary protocols and these protocols are not universally interchangeable. Before purchasing replacement detectors, modules, or notification appliances, always verify that the devices are compatible with your specific panel model and firmware version. QuickShipFire’s technical team is available to assist with compatibility verification, and our modules category includes a wide range of interface modules from leading brands to support system expansion and integration.
Sourcing Replacement Parts for Legacy Systems
Many hospitals operate fire alarm systems that are ten, fifteen, or even twenty years old. Finding replacement parts for older systems can be challenging, as manufacturers frequently discontinue products and pull them from standard distribution channels. QuickShipFire was built specifically to solve this problem we specialize in sourcing new-in-box components for older systems, including smoke detectors, detector bases, and control modules that may no longer be available from the original manufacturer’s standard catalog.
Regulatory Inspections and What Surveyors Look For
Understanding what fire safety surveyors and inspectors are looking for is a critical part of maintaining compliance. Hospital fire alarm systems are evaluated from multiple angles during regulatory visits not just whether the devices are installed, but whether they are properly maintained, correctly documented, and functionally integrated with the broader fire protection and emergency response infrastructure.
CMS surveyors conducting Life Safety Code surveys focus heavily on the physical condition of the fire alarm system, the completeness of inspection and testing records, the functionality of automatic protective actions (door release, HVAC shutdown, elevator recall), and the results of fire drills. They look for evidence that the system has been tested within the required intervals and that any deficiencies found during previous inspections have been corrected.
Joint Commission surveyors take a similar approach but also evaluate the adequacy of the facility’s fire safety management plan and the depth of staff training. They may conduct impromptu verbal assessments of staff members to gauge familiarity with RACE procedures, the location of pull stations, and the meaning of alarm signals in a zoned notification system. A well-documented, actively managed fire safety program supported by a reliable hospital fire alarm systems infrastructure is the most effective preparation for any regulatory visit.
Steps to Achieving and Maintaining Healthcare Fire Safety Compliance
A structured, proactive approach to fire safety compliance protects patients, staff, and the institution. Here is a practical roadmap for healthcare facilities:
- Conduct a comprehensive Life Safety Assessment: Engage a qualified fire protection engineer to evaluate your facility against current NFPA 101 and NFPA 72 requirements and identify gaps.
- Develop or update your fire safety management plan: Ensure the plan reflects your current facility layout, occupant population, evacuation strategy, and the capabilities of your installed fire alarm system.
- Establish a rigorous ITM program: Implement a scheduled inspection, testing, and maintenance program that meets or exceeds NFPA 72 minimums, with complete documentation maintained in a readily accessible format.
- Source and replace aging or non-compliant devices: Work with a reliable supplier like QuickShipFire to identify and replace detectors, notification appliances, or control modules that are approaching end-of-life or that have been flagged in prior inspections.
- Invest in ongoing staff training: Schedule fire drills across all shifts, conduct annual refresher training for all staff, and maintain training records that demonstrate consistent engagement with fire safety protocols.
Healthcare Fire Safety Requirements for Specific Hospital Zones
Different areas within a hospital have distinct fire safety requirements based on their occupancy characteristics, equipment hazards, and patient vulnerability levels. Understanding the zone-specific requirements for hospital fire alarm systems is essential to designing a compliant, effective fire protection strategy.
Intensive Care Units (ICUs) and Critical Care Areas
ICUs present the highest level of patient vulnerability in the hospital patients are typically sedated, mechanically ventilated, and connected to multiple lines and monitoring devices. Fire alarm activation in an ICU must trigger an immediate, coordinated staff response rather than patient self-evacuation. Alarm notification in ICU areas must be designed to alert staff rapidly without causing panic among patients who may be conscious.
Operating Rooms and Procedure Suites
Operating rooms present unique fire ignition hazards from electrosurgical equipment, laser devices, and (in some procedures) flammable prep agents. Fire alarm detection in these areas must be highly sensitive to early-stage combustion products while minimizing nuisance activations from cauterizing smoke or surgical plumes. Many facilities use aspirating smoke detection (ASD) systems in operating theaters for exactly this reason.
Laboratories and Pharmacy Areas
Hospital laboratories and pharmacies may contain flammable chemicals, solvents, and reactive materials that create elevated fire and explosion risks. These areas typically require specialized detection equipment potentially including combination smoke and gas detection and may be protected by clean agent or other specialty suppression systems that are integrated with the broader hospital fire alarm systems network.
Food Service and Kitchen Areas
Hospital kitchens operate continuously and present significant grease fire risks. NFPA 96 governs the installation and maintenance of commercial cooking equipment ventilation and fire suppression systems in these areas. Suppression system activation must be tied into the fire alarm system so that the kitchen hood suppression system’s discharge triggers an alarm signal at the control panel and automatic gas shutoff.
Don’t let compliance gaps put your facility and patients at risk. Request a quote from QuickShipFire today and let our fire safety specialists help you source the exact components your hospital needs from addressable detectors to full control panel replacements with the speed and expertise your facility demands.
Understanding Healthcare Fire Safety Requirements at a Federal Level
The healthcare fire safety requirements enforced at the federal level flow primarily through CMS’s Conditions of Participation, which reference NFPA 101 and its companion standards as the baseline. Facilities that receive Medicare or Medicaid funding which encompasses virtually every hospital in the United States must demonstrate ongoing compliance with these requirements through a combination of state health department surveys, CMS inspections, and accreditation body reviews.
The healthcare fire safety requirements landscape also includes OSHA regulations under 29 CFR 1910 Subpart E, which govern emergency action plans and fire prevention plans for general industry. Hospitals are subject to these regulations for their non-patient-care areas such as administrative offices, warehouses, and maintenance shops. Ensuring that your fire safety program addresses both the clinical and non-clinical dimensions of your facility is essential to comprehensive compliance.
Conclusion
The stakes in healthcare fire safety are uniquely high. Patients who cannot evacuate on their own, staff who must manage complex clinical situations while simultaneously responding to a fire emergency, and facilities that contain a concentration of fire hazards all create a risk environment that demands the most rigorous approach to fire detection, notification, suppression, and response. Hospital fire alarm systems sit at the center of this risk management framework, and their reliability, compliance, and maintenance are non-negotiable.
From understanding the layered framework of NFPA 101, NFPA 72, CMS Conditions of Participation, and Joint Commission standards, to selecting and maintaining the right detectors, panels, and notification appliances for each unique area of your facility, achieving healthcare fire safety compliance is an ongoing commitment that requires expert knowledge, reliable equipment, and disciplined processes.
QuickShipFire is proud to be a trusted resource for healthcare facilities across the United States, offering a broad inventory of fire alarm components from leading manufacturers all brand new in original packaging, shipped fast, and backed by over 20 years of fire and life safety expertise. Whether you need a single replacement detector or a complete system overhaul, we are here to help you protect your patients, your staff, and your institution.
Frequently Asked Questions (FAQs)
1. What code governs fire alarm systems in hospitals in the United States?
The primary code governing fire safety in hospitals is NFPA 101: Life Safety Code, specifically Chapters 18 (new construction) and 19 (existing buildings) for healthcare occupancies. NFPA 72: National Fire Alarm and Signaling Code provides the technical specifications for how fire alarm systems must be designed, installed, tested, and maintained. The Centers for Medicare and Medicaid Services has formally adopted NFPA 101 as the standard for Medicare- and Medicaid-certified facilities, making compliance a condition of federal funding eligibility.
2. Are fully addressable fire alarm systems required in hospitals?
Yes, for all new construction and major renovations in healthcare occupancies, fully addressable fire alarm systems are required. Addressable systems assign a unique identifier to every device on the network, enabling the control panel to immediately identify the exact location of an alarm a critical capability in a large, complex hospital building. Older conventional systems installed prior to current code requirements may be permitted in existing facilities, but upgrades to addressable architecture are strongly recommended and may be triggered by renovation activity.
3. How often must hospital fire alarm systems be inspected and tested?
NFPA 72 establishes detailed inspection and testing frequencies for all fire alarm system components. At a minimum, a comprehensive visual inspection must be performed annually, with functional testing of detectors, notification appliances, and control equipment at the intervals specified in NFPA 72 Table 14.4.5. Battery systems must be tested quarterly, and waterflow alarms and supervisory signals must be tested semi-annually. Complete records of all inspections, tests, and corrective actions must be maintained for a minimum of three years and made available to inspectors.
4. What is the RACE procedure and how does it relate to fire alarm systems?
RACE stands for Rescue, Alarm, Contain, and Extinguish or Evacuate. It is the standard response framework used to train hospital staff on their individual responsibilities when a fire alarm is activated. When an alarm sounds, staff must first rescue any patients in immediate danger, then activate the alarm (if not already done automatically), contain the fire by closing doors, and finally attempt to extinguish the fire with a portable extinguisher or begin evacuation as directed. The fire alarm system supports this process by providing precise location information at the control panel, automatically closing smoke barrier doors, and notifying only the affected zone to enable a coordinated, calm response.
5. What are the consequences of failing a CMS Life Safety Code survey?
Failing a CMS Life Safety Code survey can have serious consequences for a hospital’s operations and finances. CMS may issue a Condition of Participation deficiency, which requires the facility to submit a Plan of Correction and implement remediation within a defined timeline. If the deficiency is not corrected or represents an immediate jeopardy to patient safety, CMS can terminate the facility’s Medicare and Medicaid provider agreement effectively cutting off federal reimbursement, which can be financially catastrophic. Repeated deficiencies can also attract additional scrutiny and more frequent unannounced surveys.
6. Do hospitals need fire suppression systems in addition to fire alarm systems?
Yes. NFPA 101 requires automatic sprinkler protection throughout virtually all new healthcare facility construction, and the sprinkler system must be interconnected with the fire alarm system via waterflow switches. In addition to standard wet-pipe sprinkler systems, specific areas of a hospital including server rooms, MRI suites, commercial kitchens, and laboratory areas may require specialized suppression systems such as clean agent, pre-action, or dry chemical systems. Each of these suppression systems must be individually monitored by the fire alarm control panel.
7. How can a hospital source replacement parts for an older fire alarm system?
Sourcing replacement parts for older hospital fire alarm systems can be challenging, as manufacturers frequently discontinue products after ten to fifteen years. QuickShipFire specializes in finding new-in-box replacement components for legacy fire alarm systems from brands including Fire-Lite, Notifier, Simplex, Silent Knight, Gamewell-FCI, and others. Whether you need replacement smoke detectors, detector bases, control modules, or notification appliances for a system that is no longer in active production, our team can help you locate the exact parts needed to maintain your system in compliance until a full replacement can be planned and funded.